If you have been diagnosed with mitral valve prolapse, you may feel uncertain about how it will affect your life. You may wonder about your treatment options and when you’ll finally feel well again. As one of the highest volume and most experienced mitral valve repair and replacement programs in the nation, Northwestern Medicine Bluhm Cardiovascular Institute has a team of leading mitral valve experts who have answers. Your trust inspires us. Your story motivates us, and our goal is to help you feel and live better.
What Is Mitral Valve Prolapse?
Mitral valve prolapse is common. It affects up to 1 in 50 people. Most people do not need treatment because their condition is not serious.
Your heart has four sections, or chambers, that squeeze to pump blood. Valves between the chambers open and close to let blood through. The mitral valve controls the blood flow from your left upper chamber, called the left atrium, to the left lower chamber, called the left ventricle.
The mitral valve has two “leaflets,” which are sections that open and close together. If you have mitral valve prolapse, one of the valve’s leaflets does not close properly when the left ventricle of the heart squeezes. This can cause blood to flow backwards, which is called mitral regurgitation.
Mitral valve prolapse is caused by a problem with the mitral valve’s “strings,” called tendinea chordae, on the edge of the leaflet. Tendinea chordae function in some ways like the strings on a parachute. Imagine that one portion of the parachute has broken strings. When the parachute fills with air, the section without strings will not hold in the air. In mitral valve prolapse, the strings are too long or, for most patients who need surgery, several strings are broken.
Mitral Valve Prolapse Symptoms
The leaky valve can cause symptoms, especially if the leak is severe, and if it began recently. The symptoms may be mild and can include:
- Fatigue. Because some of the blood is flowing backwards, you may feel tired and lack energy. You might think, “I must be getting older.” You may have to rest more than usual.
- Shortness of breath. When the blood goes backwards into the upper chamber (left atrium), it also goes into the lungs. This can cause pressure to build in the lungs, causing congestion. Lung congestion may cause you to feel short of breath when doing physical activities, such as walking up or down stairs or hills, carrying groceries or doing laundry.
- Swelling in ankles and legs. When the pressure in the lungs becomes high, it may cause a different heart valve, the tricuspid valve, to leak. If this happens, you may have swelling in your ankles and legs.
- Atrial fibrillation. If the left atrium becomes enlarged, it may trigger an irregular heart rhythm called atrial fibrillation, or AFib. This can make your mitral valve symptoms worse. If you develop AFib, you can develop a blood clot because your atria are not squeezing as they should. If the blood clot breaks off, it can cause a stroke or another serious health event.
When patients come to surgery for severe mitral valve prolapse, about 4 in 10 have developed AFib, and about 1 or 2 in 10 have developed a tricuspid valve with a severe leak.
Surprisingly, even if you have severe mitral regurgitation, you may have no significant symptoms because you may adapt your activities, and your heart may adapt to the leak. Usually this is due to very slow worsening of mitral valve prolapse over several years. In some cases, the leak may be found only if your doctor detects a heart murmur when they listen to your heart.
Even with no serious symptoms, mitral valve prolapse is a concern because the heart adapts to a severe leak by becoming enlarged. An enlarged heart does not contract properly, causing it to become weaker. At some point, the heart can become so weak that even if the leak is corrected, the heart won’t recover. In this case, you can develop heart failure.
Mitral Valve Prolapse Diagnosis
When you have a heart valve that leaks, your doctor may hear it through a stethoscope. The sound is called a murmur. When your doctor hears a murmur, they will likely suggest you have an echocardiogram. This is a type of imaging that can help your doctor evaluate the valve and many other areas of heart function.
With an echocardiogram, your doctor can “grade” the leak. Mitral valve regurgitation is typically graded on a scale from 0 to 4:
- 0 is no leak or very minor
- 1 is a mild leak
- 2 is a moderate leak
- 3 is a moderate to severe leak
- 4 is a severe leak
Most patients who need surgery have a grade 4 leak, or in some cases a grade 3. The valve may have a grade 2 leak for years, but it is not loud enough to be heard as a heart murmur.
Treatment for Mitral Valve Prolapse
A heart valve problem is a like a mechanical failure of any valve (or the broken strings on a parachute). It doesn’t heal on its own and go away.
Medications have little effect. They may be used to reduce symptoms, for example using diuretics to remove fluid. But the valve is still “broken,” and it still leaks.
Most often, when a leak is grade 2, it is monitored closely with echocardiograms. Over time, this allows us to see if it is getting worse. Many patients may stay at this level for years.
When the leak is grade 3 or 4, especially if there are symptoms from the valve leak, then therapy is considered. Two options are:
- Transcatheter mitral valve therapy
- Surgical mitral valve repair, which is described below
Surgical Mitral Valve Repair
Surgery to repair mitral valve prolapse is generally considered to be the safest, most successful heart operation in adults. Northwestern Medicine has published the most durable results ever published for mitral valve prolapse repair.
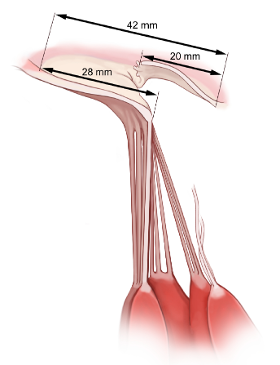
Surgeons have a variety of ways to successfully repair a mitral valve. The most common way involves removing the segment of the valve where the strings (chordae tendineae) broke.
The normal parts of the valve are then sewn back together. Other abnormal areas found in the valve leaflet are also repaired.
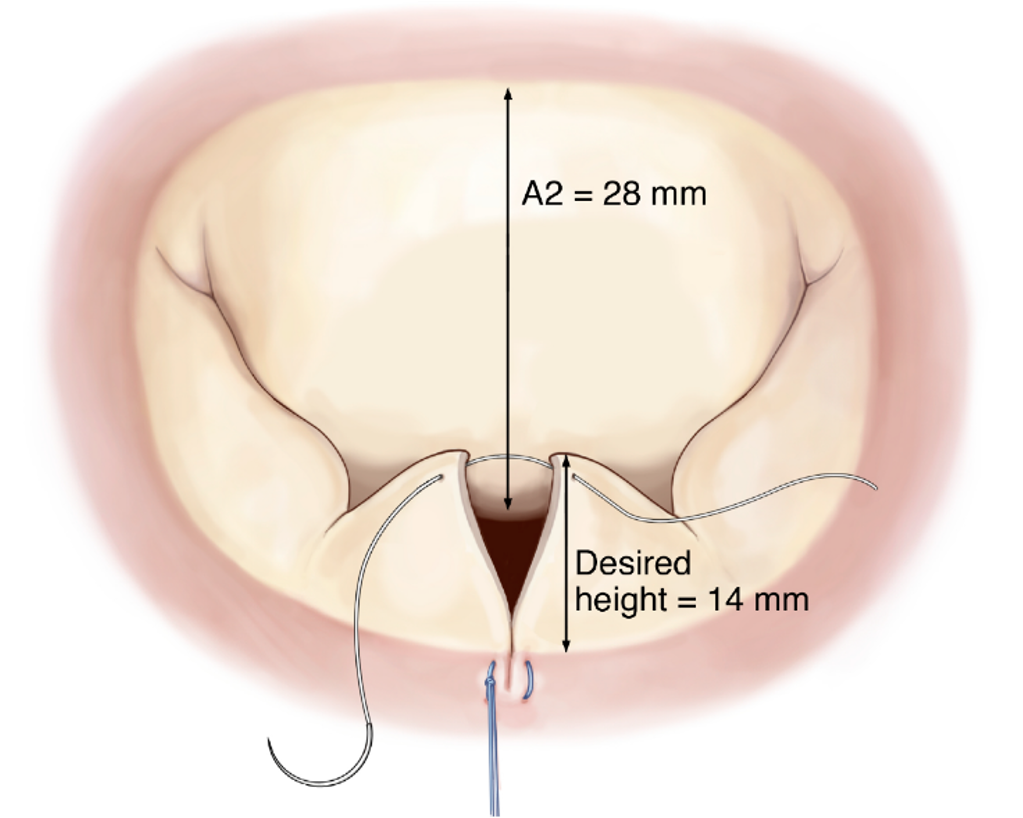
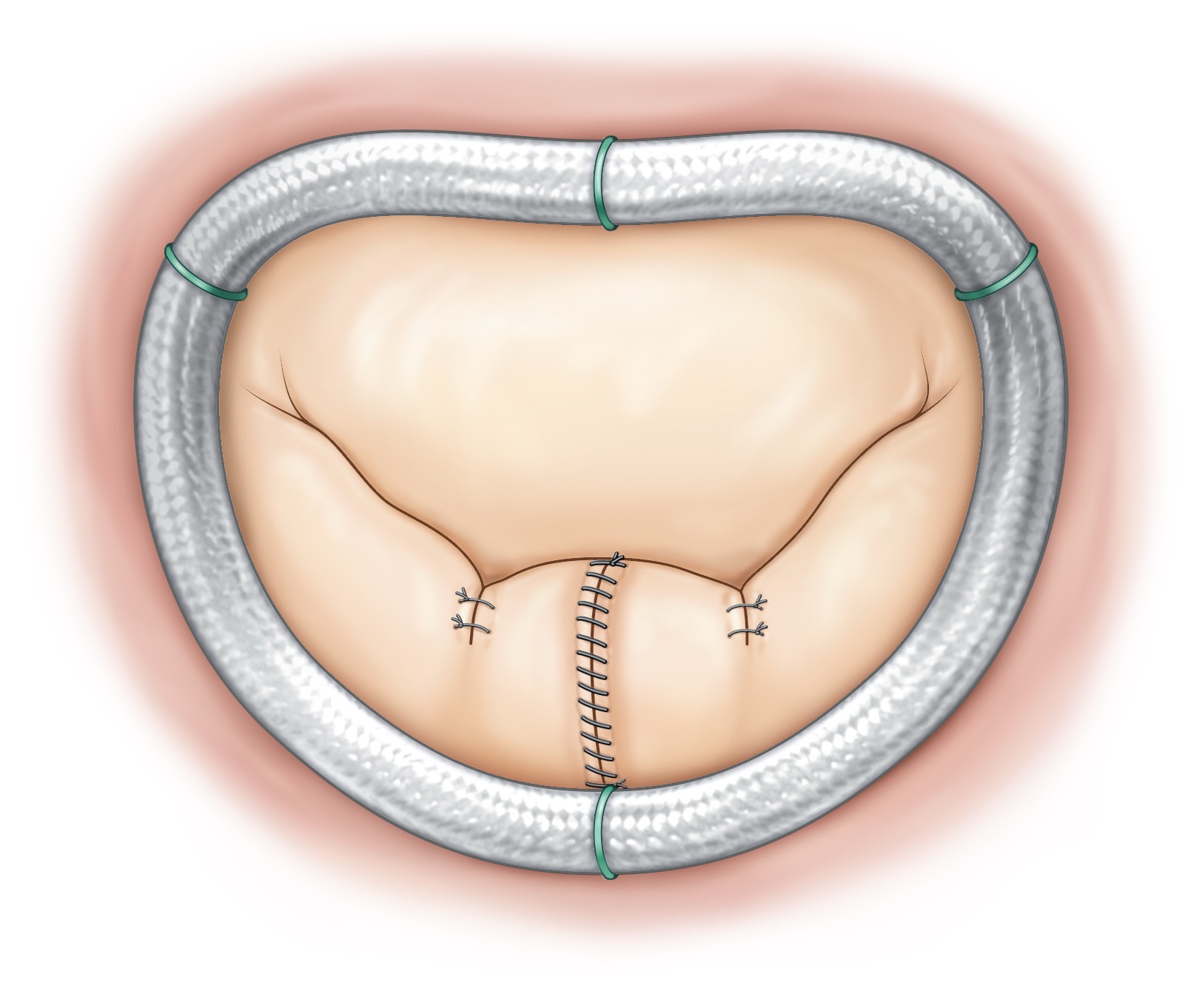
When the valve leaks, it is typically also stretched out of its proper shape. During the repair procedure, the surgeon inserts a “ring” on the edge of the valve leaflets (called the valve annulus). The ring reduces the stretched-out valve annulus and returns it to the desired size and shape so that the two leaflets close properly and support each other.
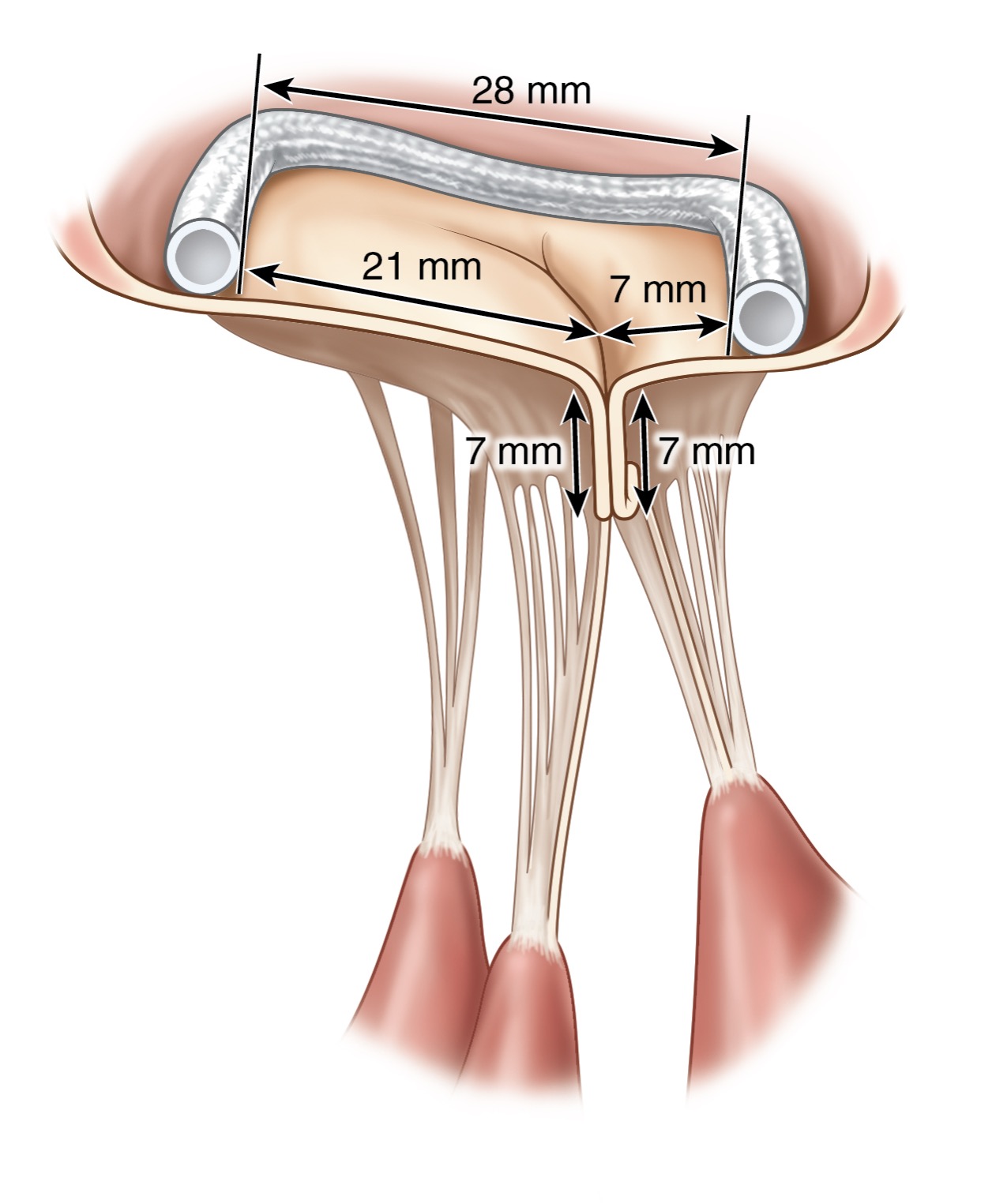
When the repair is complete, the valve is returned to its normal shape and supported by the ring. The ring becomes covered with cells so that blood thinners are not required. The goal is to ensure that the leaflets overlap the right amount — not too much and not too little. This leads to long-term ideal function.
Northwestern Medicine offers many approaches to this surgery. Patients are put on a heart-lung machine, but surgery can be done through a small incision in the middle of the chest or through small incisions in the right chest. In some cases, robotic surgery can be an option. You should discuss with your surgeon which approach is best for you. Our goal is always to choose the safest option that is most likely to give you the best long-term result.
The operation itself generally takes about 3 hours from beginning to end. That does not include time before and after surgery for anesthesia care. You will have a breathing tube during the operation, which often is removed right after surgery or shortly after you arrive in the intensive care unit (ICU).
Recovery From Mitral Valve Surgery
On a pain scale of 0 to 10, with 10 being the worst pain they have ever felt, most patients report the pain after surgery is about a 4. Your pain may be better or worse. Your care team will help you manage your pain.
Most patients move out of the ICU the day after surgery. On average, patients spend a total of four days in the hospital. Young, healthy patients may spend only three days; patients with other medical problems may need longer to recover.
Before discharge, you will be up and walking, and you will be able to go up and down steps with a physical therapist. Almost all patients are willing and able to go home after surgery instead of to a rehabilitation facility. Your care team will give you written instructions and prescriptions before you leave the hospital.
Instructions for recovery and rehabilitation are fairly simple for most patients.
- We encourage you to be up and walking around as soon as you return home.
- You can use stairs.
- You can ride in a car anytime. However, patients often feel tired for some time after surgery, so do not drive until you feel you have the energy. It takes on average about two weeks for patients to feel they can do short trips around town.
- Avoid lifting over 20 pounds for a short time. Specific guidelines will depend on the type of incision and surgical closure you had. By two to four weeks, most patients can do all daily activities and slowly increase the amount of weight they lift.
- When recovery is complete, you will have no physical limitations related to the surgery. Typically, you will not need blood thinners or other medications related to the surgery.
Most patients will never need another procedure on the mitral valve. A Northwestern Medicine study showed that fewer than 1 in 100 patients needed a second procedure by 10 years after surgery.
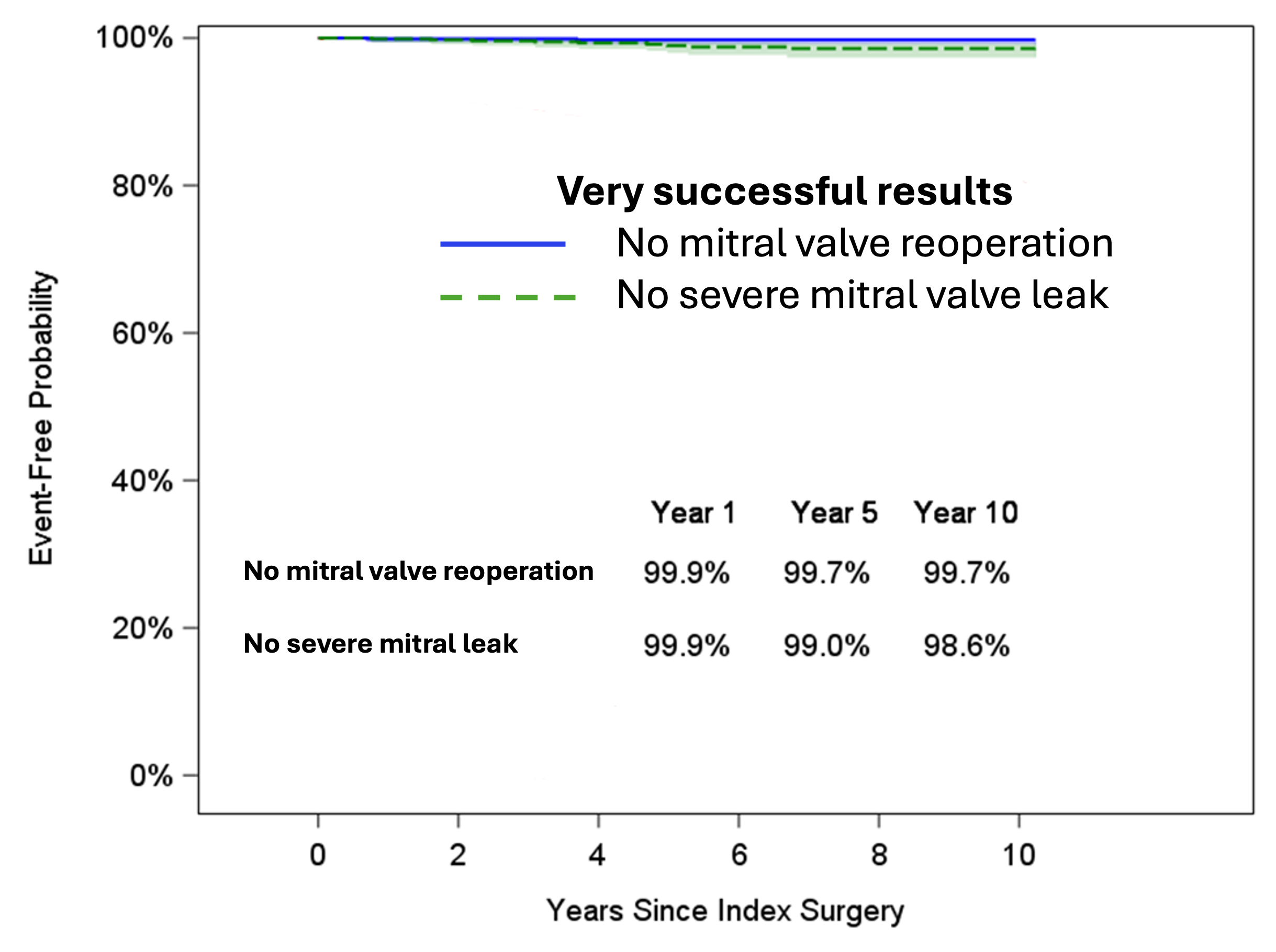
Desai A, Thomas JD, Bonow RO, Kruse J, Andrei AC, Cox JL, McCarthy PM. Asymptomatic degenerative mitral regurgitation repair: Validating guidelines for early intervention. J Thorac Cardiovasc Surg. 2021 Mar;161(3):981-994.e5.
Risks Related to Mitral Valve Surgery
Mitral valve surgery is an open-heart operation. However, the risks involved with this surgery are low. In fact, Northwestern Memorial Hospital has achieved 100% in-hospital survival for surgical mitral valve repairs.
- For routine patients, the risk of death is much less than 1 in 100. In healthy patients, it is as low as 2 out of 1,000.
- Approximately 1 out of 1,000 patients at Northwestern Medicine develops an infection after mitral valve repair.
- About 1 in 100 patients has bleeding that requires a return to the operating room (usually the day of surgery).
- Most patients do not need a transfusion.
- When a transfusion is needed, it is typically because the patient’s blood count was low before surgery.
- In general at Northwestern Medicine, mitral valve repair has a low risk of:
- Heart attack (less than 1 in 100 patients)
- Stroke (1 in 50 to 100 patients depending on their age and condition)
- Need for a pacemaker (1 in 100)
- Kidney dysfunction, mainly in patients who already have kidney disease
Videos
 5:50
5:50
