Aortic valve disease affects a large number of people of all ages, some of whom may not know they have a problem with their valve. Having a new diagnosis of aortic valve disease may be overwhelming, and choosing where to go for your care can be confusing. You may wonder about when you might need treatment and what your long-term health will look like. Maybe you are wondering how often you need to be seen, or you have been told you are “too high risk for surgery.”
We treat patients like you every day. We will be there to help you on your journey.
At Northwestern Medicine Bluhm Cardiovascular Institute, we want to make things as easy as possible for you. Through our FAST Program, you can reach our expert nurses by phone, email or online, and they will guide you to the right doctors to help you. We will help get your information, including your echocardiograms and other imaging, in our system, and then get you answers FAST, often in as little as 48 hours.
We have teams of experts who are among the best in the world at making the right diagnosis and choosing the right medical or surgical treatments for you. We have performed all types of valve surgeries, from the simplest to the most complex, and from very small incisions to operations in people who have had multiple prior procedures.
We want to partner with you for life.
What Is Aortic Valve Disease?
Aortic valve disease is common. Some forms run in families and are present at birth, and others may develop with age. The most common form of aortic valve disease affects up to 1 in 50 people.
While many people do not need treatment because their condition is not serious, it is important to understand what type of valve problem you have, and how often you should see a doctor or have testing to evaluate your valve.
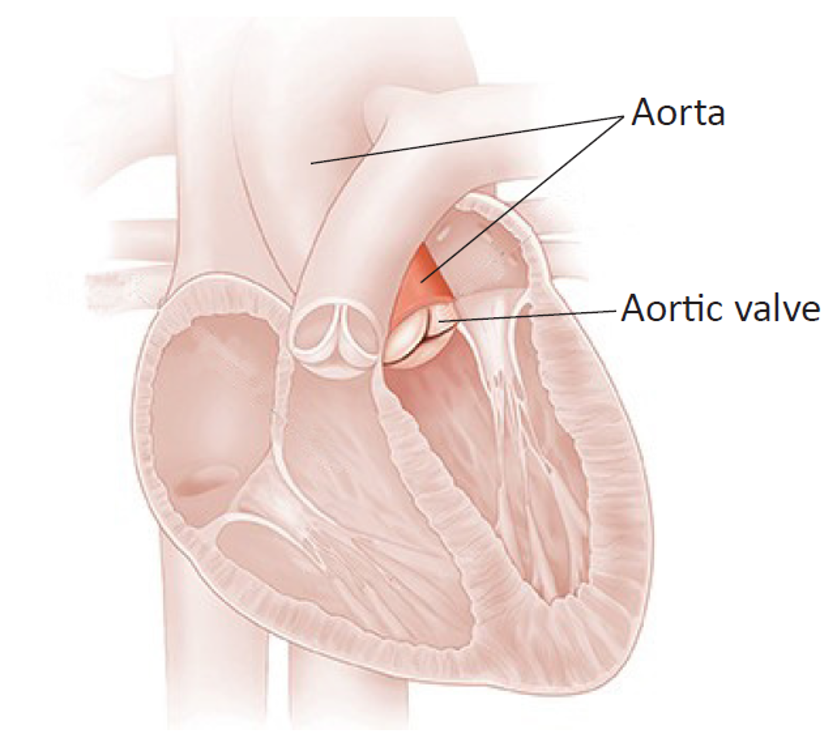
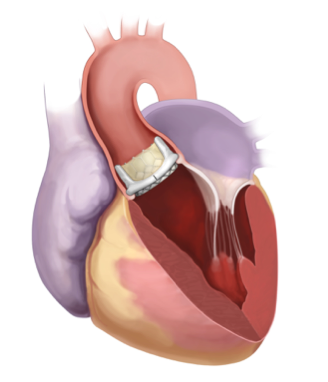
Your heart has four sections, or chambers, that squeeze to pump blood. Valves between the chambers open and close to let blood through. The aortic valve controls the blood flow from your left lower chamber, called the left ventricle, to the main artery of the body, called the aorta.
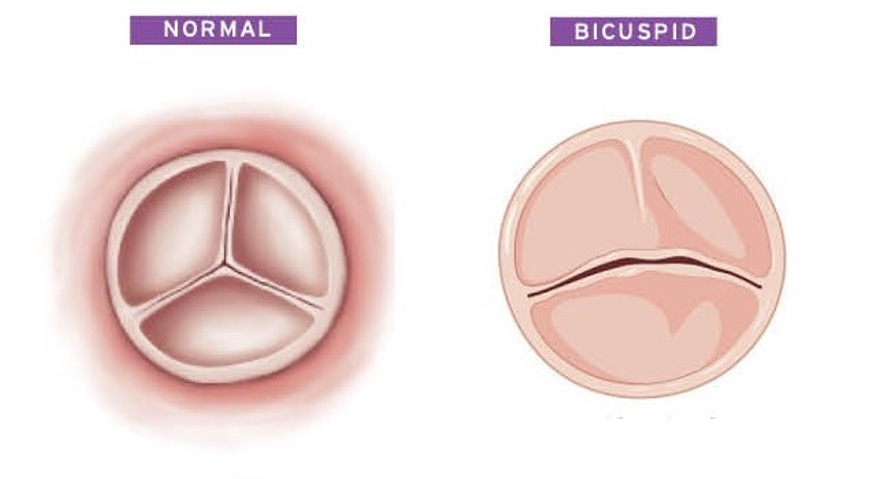
The normal aortic valve has three leaflets. They are the part of the valve which opens and closes to prevent blood from going backward into the heart between heartbeats.
©2015 Krames Staywell LLC
About 15 out of 1,000 people are born with an aortic valve that has two leaflets fused together. This is called a bicuspid aortic valve.
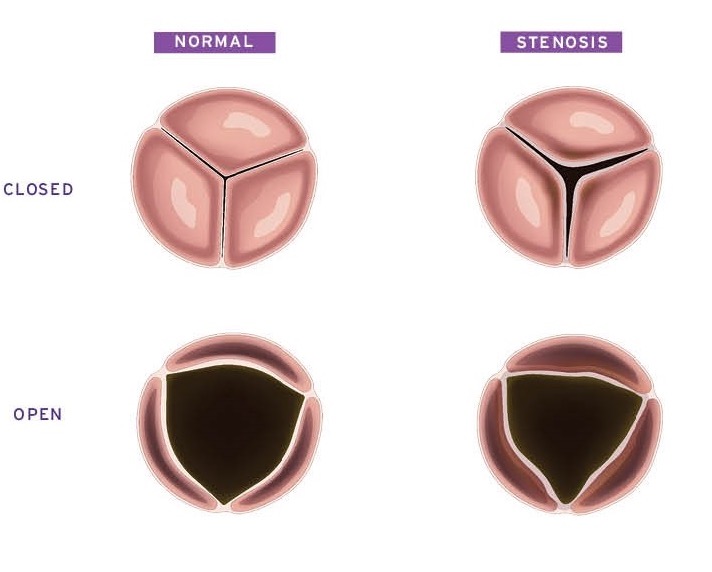
Aortic valve leaflets can become thickened and scarred. Or, in some cases, they may become floppy so they do not meet each other. Abnormal aortic valve leaflets can keep the valve from working correctly.
A valve that does not open fully prevents normal blood flow from the heart. This is called aortic stenosis.
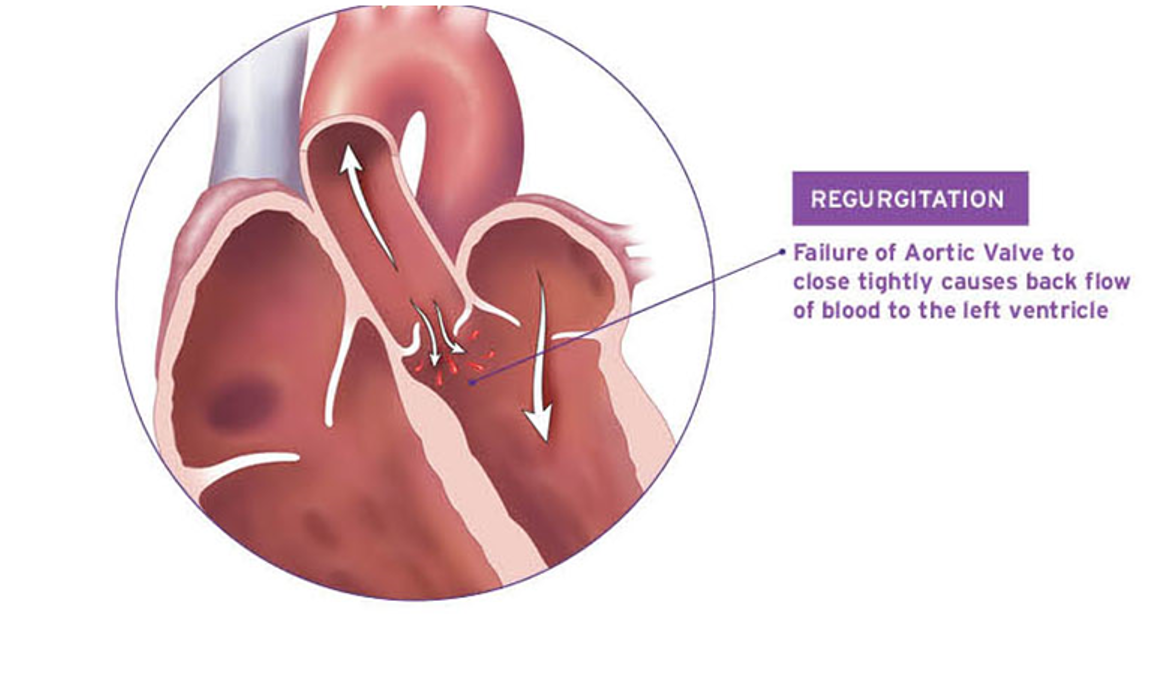
When the leaflets do not close properly, the valve allows blood to leak back into the heart between heartbeats, which is called aortic regurgitation. Sometimes both conditions happen at the same time.
Aortic Valve Disease Symptoms
An aortic valve that is narrow or leaky can cause symptoms, especially when the narrowing or leak is severe. Some patients who are otherwise healthy may have few or very mild symptoms, even when their valve disease is severe.
When they occur, symptoms may include:
- Fatigue. Because some of the blood is flowing backwards, you may feel tired and lack energy. You might think, “I must be getting older.” You may have to rest more than usual. Some patients feel OK when they are active, but become more tired at the end of the day.
- Shortness of breath. When the heart can’t pump blood out to the body normally, blood goes backward into the lungs. This may cause you to feel short of breath when doing physical activities, such as walking up or down stairs or hills, carrying groceries or doing laundry.
- Swelling in ankles and legs. When the backup of blood becomes severe, especially if there is more than one heart valve involved, you may begin to retain fluid. This can cause swelling of the ankles and legs, or in the belly.
- Chest pain. In aortic stenosis, the heart must work very hard to pump blood through the narrow valve. This can cause the heart muscle to become thickened. You may develop chest pain, pressure or heaviness with activity.
- Dizziness or passing out. In severe aortic stenosis, especially if your heart rate is fast or you are dehydrated, the heart may not be able to pump enough blood to bring normal oxygen to the brain. This can cause you to become dizzy or pass out.
Most patients have no symptoms until their aortic valve disease is severe. And even with severe stenosis or a severe leak, you may have no obvious symptoms. Your family members may notice that you seem tired or are “slowing down” before you do because the process happens slowly. In some cases, the valve disease may be found only if your doctor detects a heart murmur when they listen to your heart.
Even with no serious symptoms, aortic valve disease is a concern. The heart adapts to the valve problem by becoming enlarged or thickened. At some point, the heart can become so enlarged or thickened that even if the valve is corrected, the heart won’t recover. In this case, you can develop heart failure.
Aortic Valve Disease Diagnosis
When you have a heart valve that leaks or is narrow, your doctor may hear it through a stethoscope. The sound is called a murmur. When your doctor hears a murmur, they will likely suggest you have an echocardiogram. This is a type of imaging that can help your doctor evaluate the valve and many other areas of heart function.
With an echocardiogram, your doctor can tell how bad the leak or narrowing is. They report this with a “grade.”
Aortic valve regurgitation is typically graded on a scale from 0 to 4:
- 0 is no leak or very minor
- 1 is a mild leak
- 2 is a moderate leak
- 3 is a moderate to severe leak
- 4 is a severe leak
Aortic valve stenosis is measured in a number of ways. You may see these terms on your echocardiogram report:
- Gradient is the pressure across the valve.
- Jet velocity is the speed of blood through the narrow valve.
- Valve area is the size of the opening.
| Mean Gradient (mmHg) | Aortic Jet Velocity (m/s) | Valve Area (cm2) | |
| Normal | <2.0 | <5 | 3.0-4.0 |
| Mild | <3 | <25 | >1.5 |
| Moderate | 3.0-4.0 | 25-40 | 1.0-1.5 |
| Severe | >4.0 | >40 | <1.0 |
Your medical team will help you understand what these numbers mean. What is most important is whether you have severe narrowing of the valve.
Most patients who need surgery have a leak or stenosis that is graded “severe.” However, in some cases, patients with a moderate leak and narrowing may benefit from surgery.
Aortic Valve Disease Treatments
Surgeons and cardiologists have a variety of ways to successfully treat aortic valve disease.
- Most people with aortic valve stenosis can best be treated with aortic valve replacement, or AVR.
- Some people with aortic regurgitation, or a leaky valve, can be treated successfully with aortic valve repair.
Northwestern Medicine Bluhm Cardiovascular Institute has teams of experts with extensive experience in aortic valve repair and replacement procedures and other types of treatment. It is important to know that most patients have a choice when it comes to treatment of their valve disease. There is no “one size fits all” to treatment. We will explain your options and help you make the choice that is right for you.
Surgical Aortic Valve Replacement
During surgical aortic valve replacement, or SAVR:
- A surgeon makes an incision in the chest and opens the aorta, the main artery to the body, to get to the aortic valve.
- The diseased valve is removed.
- A new valve is sewn in place where the diseased valve was.
- The new valve will function like a normal aortic valve. It will open to allow blood out of the heart when the heart beats, and close to keep the blood from going backward in between heartbeats.
It is important for you and your surgical team to discuss what type of replacement valve will be used during your surgery.
- Tissue valves. These valves are made from animal tissue that is treated to make it last longer. Most use animal tissue that is connected to a frame made of surgical plastic and metal.
- Pros: Tissue valves do not require you to take blood thinners.
- Cons: Not all valves last the same amount of time. Your team will talk to you about how long a tissue valve is likely to last, and what options are for the future if it eventually wears out.
- Mechanical valves. These valves are made from a very pure form of carbon with a metal frame. They open and close like a pair of doors.
- Pros: They are very durable. Mechanical valves can last for decades in some cases.
- Cons: Patients need to take blood thinners for the rest of their lives.
- Stentless valves. Tissue valves without a frame are called stentless valves. These can be made of animal tissue or human cadaver tissue. While these valves are not used as commonly, our Bluhm Cardiovascular Institute team has extensive experience with using stentless valves to treat challenging aortic valve problems. For example, your surgeon may discuss using a stentless valve if:
- Your aortic valve is very small
- You have had prior valve surgery
- You have a valve infection
- Ross Procedure. In this procedure, your own pulmonary valve (the valve between the heart and the lungs) is used to replace the diseased aortic valve. This is a specialized procedure that is not performed at all centers. It can be a good choice for younger patients, and the Northwestern Medicine Ross team is dedicated to helping those patients have the best outcomes after their aortic valve surgery.
- Pros: You do not need to be on blood thinners after surgery. This can be a particular benefit for younger patients.
- Cons: This is a more involved procedure than some other forms of aortic valve replacement.
How the Ross procedure is done:
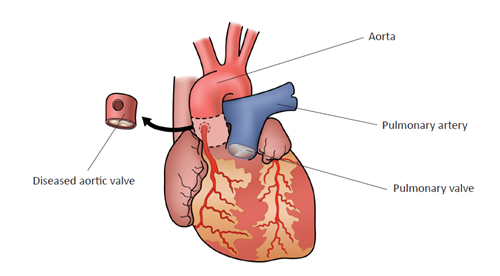
- A cardiac surgeon removes the diseased aortic valve.
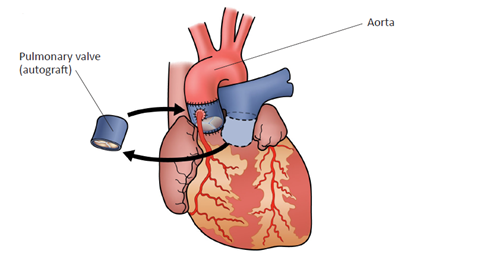
- Then, the cardiac surgeon removes the pulmonary valve and places it where the aortic valve was. After this, the pulmonary valve is called an autograft.
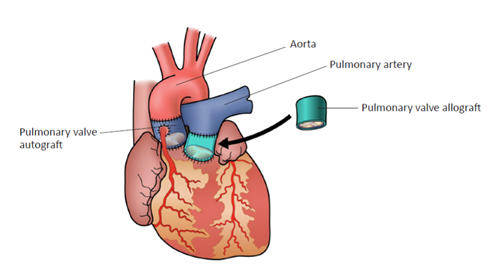
- The cardiac surgeon then places a donor valve from a human cadaver in the pulmonary valve position. After this, the donor valve is called an allograft.
Transcatheter Aortic Valve Replacement
During transcatheter aortic valve replacement , or TAVR, your surgical team will insert a tube called a catheter into your aorta, normally through one of the leg arteries. Through this tube, they will pass a new valve up inside your diseased aortic valve. The new valve is then inflated inside the existing valve.
Patients who have a TAVR procedure have a shorter hospital stay and may return to activity soon after the procedure.
Choosing the Right Valve Replacement Procedure
Whether a TAVR or SAVR procedure is right for you depends on:
- What is wrong with your aortic valve
- The size and shape of your aortic root (the area around the valve)
- Your age
- Your other cardiac conditions
- Other factors
Your specialists at Bluhm Cardiovascular Institute are here to help you understand your options and recommend which procedures may be the best fit for you.
Aortic Valve Repair
Some leaky aortic valves can be repaired. To determine if repair is possible, your surgical team will consider:
- The shape of the valve
- Whether it is a bicuspid or tricuspid valve
- Whether there is thickening
- Other factors
Surgeons have many options to repair a valve. The aortic valve repair must be tailored to the patient and the valve. While valve repair is not possible in all patients with aortic regurgitation, the Bluhm Cardiovascular Institute team has extensive experience in different repair techniques. We will explain your options based on your own valve.
Minimally Invasive Aortic Valve Surgery
Northwestern Medicine offers many approaches to aortic valve surgery. The choice of incision depends on:
- How much work is needed to repair or replace the valve
- Whether any other procedures are needed to fix other heart problems
- Whether you have had any other chest surgery
- Other factors
To help the surgical team plan the operation and choose the right incision, most patients will have a CT scan (computed tomography scan) of the chest to look at the position of the valve, the heart and important blood vessels.
Our priority is to give you the safest possible operation, with the best possible recovery.
Videos
 4:11
4:11
